The idea of “STEMI equivalents” is a response to the finding that the “STEMI/Non-STEMI” classification paradigm is inadequate for the accurate determination of patients requiring emergent revascularisation therapy. Approximately 1/4 of patients classified as a Non-STEMI are found to have total or near total acute coronary artery occlusion at delayed angiogram. These essentially represent “missed” patients who would have benefited from being “treated as a STEMI” emergently rather than in a delayed fashion.
Back in 2018 Stephen Smith, Pendle Myers and Scott Weingart published the OMI Manifesto. This document and the extensive work of Smith and Myers on the subject since seeks to replace the STEMI/Non-STEMI paradigm with an OMI (Occlusion MI)/NOMI (Non-occlusion MI) classification system. OMIs include STEMIs and so called “STEMI equivalents” that represent the same pathology – total or near total acute occlusion of a coronary artery. In a more recent 2021 Article (section 2.3) in addition to obvious STEMIs a range of OMIs are defined which include the above 4 “STEMI equivalents” published in the JACC 2022 Consensus statement, as well as several other ECG syndromes. In a retrospective case control study they found OMI ECG findings were “superior to STEMI criteria for the blinded ECG diagnosis of Occlusion MI in the hands of highly trained electrocardiographers.”
While the OMI/NOMI nomenclature have not yet been formally adopted in cardiology circles the formal recognition of STEMI equivalents effectively achieves the same purpose. However currently the list of “approved members” of this group provided in JACC 2022 is somewhat shorter than that advocated by Smith, Myers and colleagues.
Additionally, of note, the JACC consensus statement identifies the following ECG ischaemia syndromes as only indicative of “acute/sub-acute myocardial ischaemia” rather than being STEMI equivalents (NOMIs not OMIs):
- STE in aVR with multi-lead ST depression
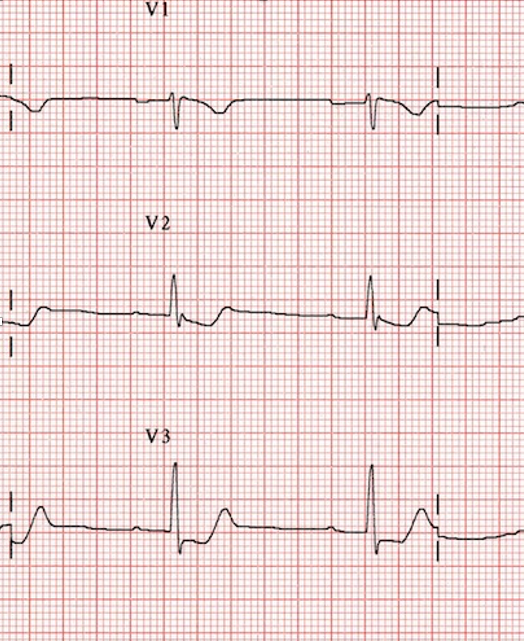
- Welllens syndrome
Such patients may still benefit from relatively urgent rather than emergent cardiology consultation which may include coronary artery evaluation.