Quick Links
– Treatment of Hypoxia and Respiratory Failure
– – NIV and HFNC
– – Intubation
– – – Airway Assessment
– – – Maximise 1st pass success
– – – Drugs
– – – Preoxygenation
– – – Re-oxygenation
– – – Apnoeic Oxygenation
Management
Management is primarily supportive care and treatment of complications.
The primary cause of mortality in COVID-19 patients is type 1 respiratory failure from several hypothesised causes including alveolar derecruitment, V/Q mismatching, ARDS and pulmonary vascular microthrombi. Consequently the Treatment of Hypoxia & Respiratory Failure will be the primary management focus of this document.
Other management considerations in COVID-19:
- There are no proven pharmaceutical treatments for COVID-19 other than supportive care. (ASID) Various candidates with low level or no human evidence of efficacy are currently being trialled around the world.
- Prophylactic anticoagulation should be considered in all patients immobilised for extended periods such as intubated patients. However evidence of microthrombi contributing to hypoxia has lead a few centres to trial therapeutic anticoagulation – results from this approach are not yet known.
- All unproven drug therapies (including therapeutic anticoagulation) are generally only recommended within the context of properly approved randomised controlled trials. [National COVID-19 Clinical Evidence Taskforce]
- Where bronchodilators are required avoid nebulisers to reduce aerosolisation of virus (ANZICS) and use metered dose inhaler (MDI) and spacer.
- Shock is uncommon though sometimes haemodynamic support is required, more often post- intubation. See Haemodynamic Support section for more information.
Treatment of Hypoxia and Respiratory Failure
Summary of Treatment of Hypoxia & Respiratory Failure Section
- Traditional recommendations for oxygenation are to target saturations above 90-92%, up to 96%. However, there are a subset of COVID-19 patients, the so called“happy hypoxics” or “silent hypoxics”, who are mentally alert despite sometimes profoundly low oxygen saturations who may warrant a different approach. [See Oxygenation Overview section]
- Prone positioning of alert patients has anecdotally been found to improve saturations and reduce work of breathing in some COVID-19 patients. [See Oxygenation Overview section]
- Initial oxygen therapy usually involves a graded escalation from low flow nasal prongs to hudson mask to non-rebreather mask (NRM) with all patients wearing a surgical mask on top of these therapies to reduce viral droplet dispersal. To reduce viral dispersal, some sources recommend transitioning from nasal prongs directly to NRM, skipping the Hudson masks. [See Initial Oxygen Therapy section]
- For patients hypoxic on 15L of oxygen via a NRM, the management options are High Flow Nasal Cannula (HFNC), Non-invasive Ventilation (NIV), intubation and palliation.
- Early in the pandemic an “early intubation approach” was the predominant advocated practice due to belief that HFNC and NIV may expose staff to greater risk of infection and be less effective. However the early intubation strategy has recently been called into question as it has seen patients intubated for very prolonged periods with high mortality. The rationale for and against the increasingly utilised HFNC & CPAP are discussed in the NIV & HFNC section.
- 2 alternative phenotypes of COVID-19 patients have been described, L (Low) & H (High). Type L patients predominate early in severe disease and appear sensitive to both Patient-Self Inflicted Lung Injury (P-SILI) (from excessive work of breathing) and high positive pressure injury (from high PEEP CPAP, BiPAP and ARDSnet mechanical ventilation). There have been resultant recommendations for changes in management [see Oxygenation Overview section] . This includes:
- High FiO2, intermediate PEEP non-invasive strategies (HFNC and CPAP) titrated more to reducing excessive work of breathing than oxygen saturations per se.
- Where this is unsuccessful, early intubation is advised over prolonged non-invasive strategies.
- Upon intubation, a marked deviation from the previously recommended high PEEP ARDSnet, “lung protective” ventilator protocols towards a high FiO2, intermediate PEEP strategy in type L patients. [see Post Intubation Care section]
- Where intubation is indicated, there are numerous modifications required to the peri-intubation process for suspected COVID-19 patients to maximise staff safety. [See Intubation section]
Oxygenation Overview
Rapid evolution of recommended COVID-19 management is emerging from the epicentres of the pandemic (Gattinoni 2020, EMRAP live 31/3/20 & 7/4/20, EMCRIT Wee 30/3/20, REBELCast 5/4/20 EM Cases COVID Update 5/4/20). This section incorporates these new advances into the management paradigm.
Standard recommendations generally suggest hypoxic patients should be provided oxygen therapy by the lowest Fi02 method capable of providing saturations that are greater than 90-92% and no higher than 96%. (SSC, IPCC19, ASID)
However, some surprising peculiarities in the presentation of COVID-19 patients and the management of their hypoxia have been described:
- Permissive Hypoxaemia: A unique syndrome of COVID-19 patients has been described (the so called “the happy hypoxics” or “silent hypoxics”) who are mentally alert and lack significant respiratory distress despite hypoxaemia that would usually prompt treatment, sometimes with profoundly low oxygen saturations.
- It has also been theorised that given the lack of distress in some profoundly hypoxaemic patients, that COVID-19 may interfere with oxygen saturation measurements possibly through affects on haemoglobin however while this may play a role, there are anecdotal reports that blood gas arterial oxygen measurements still roughly correlate with oxygen saturations.
- Altered triggers for escalation of oxygenation therapies: It has been suggested that a less aggressive escalation of care through progressive non-invasive and invasive therapies may be uniquely warranted in these patients. Decisions to escalate oxygenation therapies may need to be based less rigidly on measured oxygen saturations and respiratory rate per se and instead more closely based on reduced mental alertness and excessive work of breathing.
- Awake Proning: While proning has been suggested for intubated patients, recent anecdotal reports suggest symptomatic improvement from encouraging self-proning as well as repositioning in other positions (e.g. lateral recumbent, seated) in cooperative, awake patients. A CARP (COVID Awake Repositioning/Proning Protocol) has been suggested by emcrit.

Awake proning in the “happy hypoxic” on her smartphone. Source: @EricLeeMD
Titrated oxygen therapy is usually provided in a graduated fashion via low flow nasal prongs (0.5-4L/min) → Hudson mask (4-8L/min) → non rebreather mask (10-15L/min). To reduce viral dispersal, some sources recommend transitioning from nasal prongs directly to NRM, skipping the Hudson masks. [See Initial Oxygen Therapy section]
For patients hypoxic on 15L of oxygen via a NRM, the management options are:
-
- High Flow Nasal Cannula (HFNC)
- Non-invasive Ventilation
- Intubation
- Palliation
The Early Intubation Strategy Needs Modification
Early intubation has been the predominant paradigm early in the pandemic due to a belief that non-invasive strategies resulted in high infection risks to staff and were relatively futile in avoiding intubation (see NIV & HFNC section for full discussion). However there is no evidence that choosing early intubation instead of NIV or HFNC improves outcome. In fact, early reports from the epicentres of the pandemic suggest intubated patients remain on ventilators for extended periods, often fail extubation requiring re-intubation and mortality rates appear to be high. There were initial sporadic reports suggesting mortality of intubated patients to be between 50-90% and more recently a large published cohort of 2634 hospitalised patients in New York, found a very high mortality of 88% in intubated patients (76% under 65y.o and 97% over 65y.o). The cohort represents patients admitted from 1st March and the mortality data was from those who had completed care by 4th April (death or discharge) so it is likely (though not definite) that the majority of those were managed during a period when the “early intubation” approach was prevailing. (Richardson JAMA 22/4/2020)
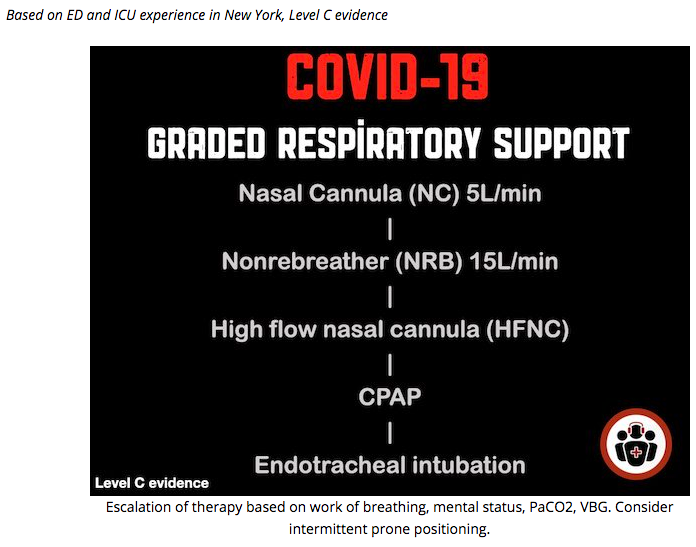
Suggested graded respiratory support progression from EM Cases COVID-19 Updates 5/4/20
For discussion regarding how to maximise staff safety see NIV & HFNC section
Intubated patients are thought to pose lower risk of viral dispersion to staff as they are ventilated via a closed circuit without leak. However both the process of intubating and extubating are high risk to staff and there are reports of accidental ventilator circuit disconnection when intubated, particularly when patients are transported out of ED. There is some uncertainty regarding the comparative risks to staff of NIV & HFNC – both can be minimised depending on equipment available and set up (see NIV & HFNC section).
Consequently, and combined with the knowledge yielded from revelation of distinct L & H patient phenotypes (see below) practice in the pandemic epicentres has moved towards the carefully measured use of HFNC and/or CPAP (titrated more to work of breathing rather than oxygen saturations per se), and alternate ventilator settings when intubated (see Post Intubation Care section). Guideline recommendations are now also changing – UK NHS guideline 6/4/20 recommends CPAP and the US National Institute of Health (NIH) guideline 21/4/20 which involved numerous relevant organisations including the American College of Emergency Physicians recommends a trial of HFNC over NIV and if HFNC not available, to trial NIV. Measures of trial success and when to covert to intubation are discussed below.
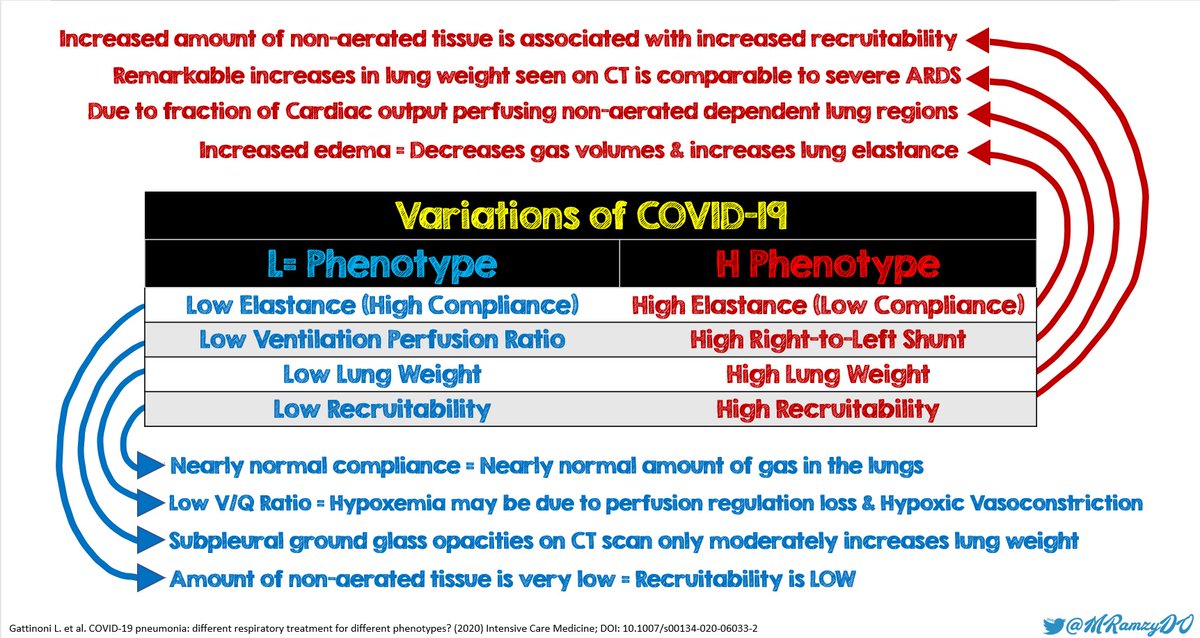
L & H Phenotypes
Luciano Gattinoni, a world expert in ARDS, has released a series of landmarks papers (ICM 2020, Critical Care 2020, JAMA 2020), detailing how the Italian experience has revealed 2 very different phenotypes of COVID-19 patients with severe hypoxia, described as the L (Low) and H (High) phenotypes. The H phenotype is typical of usual ARDS patients with high lung weight from oedema and resultant alveolar derecruitment and may benefit from the recommended high PEEP ARDSnet ventilator protocols to aid recruitment. However it appears that most patients start as the L type (and may transition to the H type) and while severe hypoxia is also a feature, this is thought to be caused by several alternative factors including V/Q mismatching due to pulmonary vasoplegia (causing loss of hypoxic pulmonary vasoconstriction) and pulmonary vascular microthrombi as well as relatively low levels of interstitial oedema & alveolar derecruitment.
Excessive work of breathing causes lung injury
It has been previously described (Brochard, 2017) that in the awake spontaneously breathing patient where their increased work of breathing is excessive, accompanying the high tidal volumes is high negative intra-thoracic pressure swings . When this is combined with increased lung permeability due to inflammation, it results in interstitial lung oedema. This process is known as Patient Self-Inflicted-Lung Injury (P-SILI).
It is currently theorised that in the type L patients with low resistance-high compliance lungs, prolonged periods of excessive work of breathing may be causing P-SILI. Combined with innate disease progression in COVID-19, this results in type L patients transitioning (gradually or sometimes precipitously) to the H phenotype as lung oedema increases to a critical mass causing derecruitment of alveoli.
It is also thought that type L patients are sensitive to high positive pressure lung injury from strategies including high PEEP CPAP, BiPAP and mechanical ventilation with ARDSnet strategy.
Consequently, balancing the risks of P-SILI and high positive pressure lung injury has resulted in a suggested middle ground, where the strategy of oxygenation therapy in COVID-19 patients with severe hypoxia should be to:
- First trial “high FiO2/intermediate PEEP”, non-invasive strategies such as HFNC and/or CPAP with the primary aim of reducing excessive work of breathing and consequently avoid P-SILI.
- Implicit in this strategy is a “Permissive Hypoxaemia” approach where “reasonable saturations” are accepted (where usual sats targets are not achieved) as long as the work of breathing goal is achieved and mentation is intact. However specific alternative minimum saturation targets have not been determined, partly it seems due to high variation between patients.
- If this is not successfully achieved, intubation should then occur.
It is thought that executing this “modified early intubation strategy“in these patients who have failed non-invasive strategies by this measure may consequently reduce lung injury and transition to the H phenotype with attendant higher mortalities. Furthermore, upon intubation of said patents, an alternative high Fio2/intermediate PEEP/ moderate tidal volume strategy has been advocated (see Post Intubation Care section).
Where the decision is made to intubate, there are numerous modifications required to the peri-intubation process to maximise staff safety. [See Intubation section]
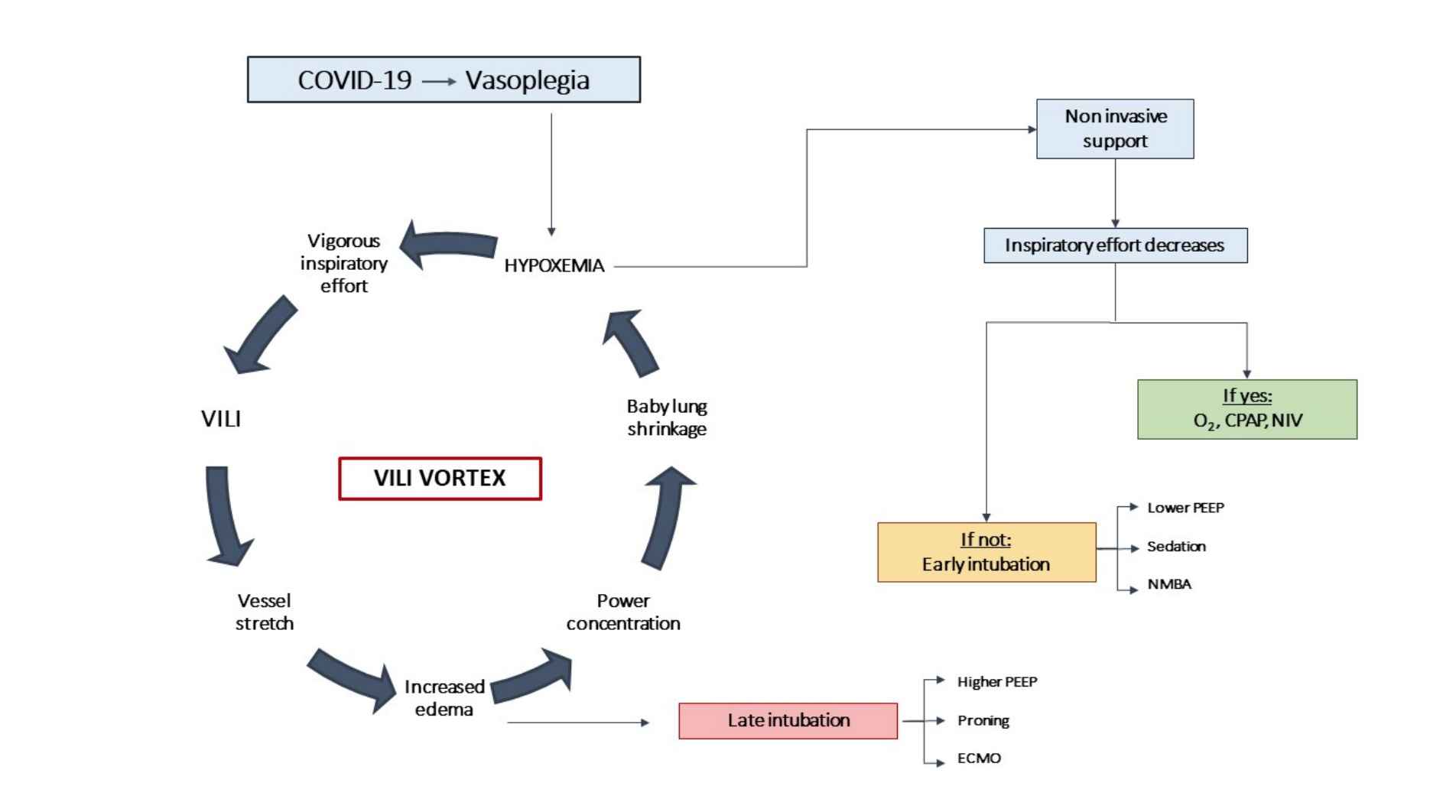
Avoiding the vortex of lung injury from excessive work of breathing using NIV and then early intubation only if this fails to curb respiratory effort.
Source: Marini & Gattinoni, JAMA 2020 PMID 32329799
Initial Oxygen Therapy
Titrated oxygen therapy is usually provided in a graduated fashion via low flow nasal prongs (0.5-4L/min) → Hudson (simple) mask (4-8L/min) → non rebreather mask (10-15L/min).
Where nasal prongs are used alone, always place a surgical mask on the patient. The placement of a surgical mask over the top of Hudson and non-rebreather masks (NRM) are likely to enhance staff safety as well.
There is evidence that viral dispersion risk is substantially reduced with NRM (10 cm dispersion) compared with both nasal prongs and standard oxygen masks (40cm dispersion) (Hui 2014). This has lead some sources to recommend that patients who are hypoxic on low flow nasal prongs should be transitioned directly to NRM, skipping Hudson masks entirely. (ACEM – Treatment) However if surgical masks are placed over all masks, it is unknown if any difference in viral dispersion would remain.
These oxygen therapies do not qualify as AGPs and consequently PPE appropriate for routine care is appropriate. (ANZICS, SAS, WHO, ACEM, Aus DOH PPE)
Non Invasive Ventilation (NIV) and High Flow Nasal Cannula (HFNC)
Summary:
- There is great controversy and uncertainty regarding both the safety and efficacy of NIV and HFNC in COVID-19 patients and a paucity of quality evidence to guide decision making. The risk-benefit of non invasive versus invasive strategies in terms of risk to staff and the benefit to patients is unknown. Consequently no clear evidence based recommendations can be made regarding whether to use NIV, HFNC or to choose an early intubation strategy. Early in the pandemic, guidelines and opinion favoured an early intubation strategy but further anecdotal experience from epicentres of the pandemic now questions this approach.
- NIV
- NIV aerosolises virus, may fail to prevent intubation in the majority of patients and extended therapy possibly contributes to alveolar pressure injury.
- Where NIV is used, CPAP is the preferred modality over BiPAP as it is the preferred therapy for type 1 respiratory failure and is theoretically less likely to attend the same level of risk of alveolar pressure injury and disease aerosolisation that has been attributed to NIV generally (which is often in reference to BiPAP).
- CPAP has recently been recommended for COVID-19 patients in the UK (NHS Guideline)
- Where NIV is used, it should ideally be used with a closed-circuit system with a high efficiency viral filter between mask and the circuit.
- HFNC
- There are mixed recommendations regarding it’s use in COVID-19 due to consumption of oxygen supplies and uncertainty regarding whether it aerosolises virus significantly or avoids intubation.
- If used, place a surgical mask on the patient.
- HFNC with attendant surgical mask has potential benefits over NIV in terms of possible reduced infection risk to staff, improved patient comfort and easier ability to enact other strategies such as patient’s self-proning.
- The decision to use NIV or HFNC versus early intubation or palliation may depend on a range of patient and hospital specific factors detailed below.
- Any attending staff to a patient on NIV or HFNC should wear PPE appropriate for AGPs and the procedure should ideally occur in single negative pressure rooms if available.
There is controversy and limited evidence regarding the use of NIV and HFNC in COVID-19.
NIV
NIV has questionable utility in viral pneumonia/pneumonitis. Studies with NIV used for Influenza A (H1N1) found that NIV failed in 57-85% of patients (Kumar 2009, Rodriguez 2017). Additionally a study of MERS coronavirus outbreak found 92% of patients initially managed with NIV required intubation (Alraddadi 2019). However in one small case series of patients with COVID-19 in Wuhan, only 48% of patients started on NIV required intubation (Yang 2020) which is somewhat more promising, albeit based on very limited numbers.
There are also concerns that NIV may aerosolise virus and spread disease to staff and other patients, however the extent of this will depend on the type of equipment being used. If the NIV has a closed-circuit set up which involves the expiratory limb tubing feeding back into the machine (typically a ventilator rather than a stand alone NIV machine) and a high efficiency viral filter is used between mask and expiratory limb, then the risk is reduced to the mask leak (which should be actively minimised as much as possible). If this closed-circuit set up is not available, expiration will generally be venting to room air and is high risk of disease spread.
Given concerns re the futility of NIV and the risk of disease spread to staff, the routine use of NIV (especially BiPAP) has typically not been recommended by several sources, in the care of suspected COVID-19 patients with respiratory failure.
Unfortunately most evidence and discussion regarding NIV, groups CPAP in together with BiPAP despite much of the data being in reference to BiPAP. There are strong theoretical grounds that CPAP may be a preferable treatment as it is the preferred NIV mode for type 1 respiratory failure and attends reduced mean airway pressures and theoretically reduced risk of viral aerosolisation. CPAP has recently been specifically advocated for the care of COVID-19 patients in the UK (NHS guideline). The helmet-mask interface theoretically has lower risk of air leak and potentially improved comfort, is used extensively in Italy and has been recommended by some sources (IPCC19) but this is currently not widely available in Australian healthcare.
Where NIV is commenced it should generally be exclusively CPAP, unless the patient is fatiguing or acutely hypercapnic; in such patients consider early intubation unless presenting with an acute on chronic BiPAP responsive condition (e.g. COPD) where BiPAP may be more rationally considered.
HFNC
Some sources recommend against HFNC because of concerns that it may increase viral aerosolisation, fail to prevent intubation and consume oxygen supplies (NHS Guideline, IPCC19), while other sources recommend it as a therapy since newer, well fitted HFNC systems are thought to have a relatively low risk of aerosolisation with potential to avoid intubation (ANZICS, SSC, WHO, ACEM). There is little high quality evidence to resolve this debate.
Regarding infection risk, one small study found no difference in bacterial aerosolisation between HFNC at 60L/min and oxygen face mask therapy. (Leung, 2019)
Regarding efficacy, in one small cohort study of 25 patients with severe influenza A/H1N1 infection, HFNC was successful in 45%, with severe patients eventually requiring intubation. (Rello, 2012) For COVID-19, a small cohort from Chongqing, China recently demonstrated that of 17 patients treated with HFNC for severe disease, 7 (41%) experienced treatment failure and were transferred onto NIV. Of these 7, 2 (29%) required eventual intubation which reveals a very low 12% rate of overall treatment failure from a sequential HFNC/NIV approach. (Wang, 2020). Notably though, selection bias may exaggerate any benefit of HFNC in these small non-randomised trials.
Where HFNC is used, a surgical mask should also be placed on the patient – this should theoretically substantially reduce viral dispersal, and there is some evidence in support of this though the source is an industry sponsored analysis of a slightly different technology which lacks peer review (Vapotherm Report).
HFNC with attendant surgical mask has potential benefits over NIV via an NIV mask:
- As explained above, it is unclear if HFNC significantly aerosolises virus and if it does this may be substantially ameliorated by the wearing of a surgical mask.
- Patients are often more comfortable on HFNC, not requiring repeated attendances for NIV mask comfort issues or requesting breaks from wearing the NIV mask which comparatively could reduce disease spread to staff with HFNC,
- Patient’s are more able to change position and self-prone.
Given concerns regarding disease spread, possibly high failure rates of NIV and HFNC, and potential risks of alveolar pressure injury from NIV early in the pandemic, guidelines and opinion were mixed in their recommendations with most advocating against NIV, with a diversity of opinion on HFNC. It had been suggested that for patients who are unable to maintain saturations on a non rebreather mask they should be considered for early intubation or palliation, though the lack of quality evidence makes the validity of this binary decision making unclear.
Notably, there is no evidence that choosing early intubation instead of NIV or HFNC improves outcome: intubated patients remain on ventilators for extended periods and mortality rates appear to be high in intubated patients. The intubated patient is thought to pose lower risk of viral dispersion to staff. However both the process of intubating and extubating are high risk to staff and there are numerous reports of accidental ventilator circuit disconnection when intubated, particularly when patients are transported out of ED. Both the overall risk to staff and benefits to patients of an early intubation strategy compared to the use of NIV or HFNC are unknown. Recent anecdotal experience from epicentres of the pandemic now questions the early intubation approach. (EMRAP live 31/3/20, 7/4/20, EMCRIT Wee 30/3/20, REBELCast 5/4/20 EM Cases COVID Update 5/4/20)
Even if NIV and HFNC are generally avoided within an ED, complexities will occur in the management of patients with possible alternative diagnoses who may or may not have COVID-19. E.g. acute pulmonary oedema patients are usually very successfully treated with CPAP and would be clinically disadvantaged by early intubation.
In patients who remain hypoxic on face mask oxygen, the decision to utilise NIV or HFNC instead of proceeding straight to intubation or palliation may depend on a range of factors:
- Patient specific factors such as disease severity, age and co-morbidities
- Likelihood of COVID-19 or other viral pneumonia versus alternative respiratory diagnoses
- Hospital resources including:
- Available types of PPE
- COVID-19 specific intubation team training level
- Current and predicted ability to geographically isolate patients in a single room and/or negative pressure rooms and/or cohort COVID-19 patients together
- Types of equipment e.g. closed circuit NIV with viral filter, newer well fitting HFNC
- Availability of ventilators – NIV/HFNC may be used to delay intubation in a stressed system where ventilators are not currently available.
- Evolving evidence of spread of disease to health care workers within the institution using these different methods.
Intubation
There are a number of alterations to the usual peri-intubation process that need to be made in order to minimise the risk of infection to attending staff. While there remains some resistance to the routine use of intubation checklists in EDs, as COVID-19 intubations represent a significant deviation from routine practice with high risks to staff, the use of a purpose designed COVID-19 intubation checklist should be considered mandatory in every department. Additionally, frequent and repeated simulation is recommended for staff training for what is a complex, unfamiliar and high stress clinical scenario.
Given the added complexity of the peri-intubation process and the need for the intubation team to carefully don PPE, the pre-intubation preparation period can take significant time. Consequently decisions regarding intubation need to be made early, as the team will not be able to safely intervene to intubate a crashing patient.
The peri-intubation process is high risk for aerosol generation. PPE appropriate for AGPs is required by all staff in the room and some centres use additional precautions (see PPE for “highest risk” AGPs), especially for the intubator at the highest risk. If practical and available use a single room, ideally a negative pressure room. Limit staff present at tracheal intubation to one intubator, one airway assistant and one to team lead/administer drugs/monitor patient (COVID-19 AMP) together with 1-2 “runners” positioned immediately outside the room, to provide additional assistance if and when required. Where an “ante room” exists connected to a negative pressure room used for intubation, ideally 1 “door” runner” (“dirty runner”) should be stationed within this also wearing PPE appropriate for AGPs, while an “outside room” runner (“clean runner”) stands outside of the ante room to source equipment and drugs that are unexpectedly needed and pass them to the “door runner”.
There is a balance between bringing into the room as much equipment that is most likely required for intubation safety and needing to minimise the amount of equipment that is contaminated by entering the room that will need to be either cleaned or discarded post intubation. Consequently backup safety equipment that has a low chance of being used, like a hyper-angulated video laryngoscope blade or cricothyrotomy equipment, may be best left outside the room in the “clean” area but still readily available if called for.
It is critical that departments ensure that all viral filters used for NIV or the peri-intubation period are rated as high efficiency viral/bacterial filters with >99.9% filtration. Viral filters can be stand alone filters or can be HME (Heat Moisture Exchange) filters with high efficiency viral filtration properties. However some HME filters do not have these required properties so this must be confirmed before stocking in critical care areas.
Airway Assessment
A standard ED airway assessment should be performed as permitted by patient clinical state and performed from as distant a position from the patient as possible. However awake intubation for predicted difficult intubation is not advisable due to high risk of disease spread. If difficult intubation is predicted, consider alternatives such as “priming” for CICO Rescue (Can’t Intubate, Can’t Oxygenate) prior to delivering pre-intubation sedation/paralysis i.e position person at the patient’s neck fully prepared as per the Vortex CICO status “SET”.
Epicentre anecdotes report a high number of patients with pharyngeal oedema above the cords on intubation with some difficulty passing a flexible bougie and the use of a less flexible stylet type introducer being suggested as an alternative. (EMRAP live 31/3/20)
Maximise 1st pass success
- All standard of care aspects of optimal intubation management should be employed to maximise first pass success.
- Specifically, this should include using the most capable intubator who is readily available to intubate (COVID-19, AMP, ANZICS, SAS) and using video laryngoscopy (VL) (ANZICS, SAS). Additionally VL can allow the intubator to maintain a greater distance from the patient’s mouth to reduce disease spread. (SAS)
Drugs
Give a high dose paralytic to ensure adequate and rapid paralysis to minimise the length of the apnoeic period and to reduce risk of coughing in the peri-intubation period for staff safety.
There is no consensus on dosing but Suxamethonium 1.5mg-2mg/kg or Rocuronium 1.5mg/kg have been suggested. The standard 1.2mg/kg dose of rocuronium is arguably most appropriate for the rapid sequence intubation of well patients – in unwell patients higher doses have been suggested to absolutely minimise the risk of coughing and ensure rapid paralysis.
Some advocate rocuronium as the preferred choice over suxamethonium as for the former, the lack of muscular fasciculations (with attendant reduced muscular oxygen consumption) may prolong time to desaturations while the longer period of paralysis further reduces the risk of coughing in the peri-intubation period.
In haemodynamically unstable patients ketamine is the sedation drug of choice. However even in the stable patients, ketamine could still be argued to be the preferred agent, for if the patient does not cooperate with preoxygenation, ketamine can be administered prior to intubation as part of a DSI (Delayed Sequence Intubation) approach – dissociative procedural sedation to enable preoxygenation. Even if ketamine is not chosen as the preferred intubating agent, it should be taken into the room to enable DSI if required.
Preoxygenation:
Summary:
- Most suitable preoxygenation options within ED’s are the Bag Valve Mask (BVM) with PEEP valve or the Mapleson C circuits.
- For most EDs, using a BVM with a PEEP valve is likely to be the most practical and familiar option for the ED provider.
- Regardless of device choice, modifications are required to maximise safety including holding the mask with a 2 handed approach, attaching a viral filter between the mask and the rest of the equipment and avoiding positive pressure ventilations where possible.
- VAPOX protocol (Ventilator Assisted Preoxygenation) has strong theoretical benefits for the intubation of patients who remain hypoxic on NRM but it is not recommended for preoxygenation of COVID-19 patients. For more information click here.
- Minimise the interval between removal of patient’s protective mask and the application of the BVM (or Mapleson) connected face mask with viral filter attached. (SAS)
- A minimum of 5 minutes of preoxygenation is recommended to fully pre-oxygenate the patient.
- Some sources suggest to depressurise the circuit (remove PEEP) during the apnoeic period, prior to removal of the face mask from the patient and before the intubation attempt to reduce the risk of viral dispersal from chest deflation.
Patients who are hypoxic on face mask oxygen are at higher risk of mortality on intubation if they are not optimised prior to intubation. Consequently a preoxygenation device with a low risk of viral dispersal to staff and that can provide PEEP will be required. Additionally for simplicity the same device should generally be used for re-oxygenation (see below) between intubation attempts.
The most suitable options for preoxygenation within ED’s are the Bag Valve Mask (BVM) or Mapleson C circuits. (SAS) For both options, key requirements include:
- Placing a viral filter between the mask and the rest of the equipment
- The viral filter should be applied directly to the face mask as an increased number of connections between the face mask and filter increase the opportunity for disconnection on the patient side. (SAS)
- Monitoring continuous waveform capnography (SAS) by placing a CO2 monitor between viral filter and the rest of the device or (ideally) attaching a CO2 sampling line to the viral filter (if such equipment is available). A triangular rather than a square CO2 trace or a low numerical value can indicate mask leak (SAS) and being pre-attached can remove a task required post intubation before connecting to the ventilator.
- Using a 2 hand grip on the mask to minimise face mask air leak. (SAS)
- Generally avoiding positive pressure manual ventilation during preoxygenation. During the post-paralysis apnoeic period, patients with severe disease may require manual ventilation to prevent profound desaturation. To minimise the risk of aerosolisation of airway secretions, this should be performed as a two person technique, with the airway assistant gently squeezing the bag and adjusting the level of PEEP as required. (SAS)
For most departments, the simplest and most familiar option would be to use the Bag Valve Mask (BVM) as the preoxygenation device with a PEEP valve attached to provide PEEP.
The Mapleson C circuit is an alternative that can deliver PEEP and has the advantage of bag deflation providing an indication of mask leak. However it is generally not widely available or commonly utilised in EDs.
VAPOX protocol (Ventilator Assisted Preoxygenation) has strong theoretical benefits for the intubation of patients who remain hypoxic on NRM. However for COVID-19 there are a number of modifications that need to be made to ensure staff safety that both increase cognitive load in a high stress situation and reduce some of the usual benefits of VAPOX protocol. Consequently it is not recommended for COVID-19 preoxygenation. For more information see the addendum at the end of this post.
Minimise the interval between removal of patient’s protective mask and the application of the BVM or Mapleson connected face mask with viral filter attached. (SAS)
A minimum of 5 minutes of preoxygenation is recommended to fully pre-oxygenate the patient.
At the end of the post-paralysis apnoeic period, when the preoxygenation device is removed from the patient, the deflation of the lungs (that were splinted under the pressure of PEEP) exposes staff to additional risk of viral dispersal. The level of risk this affords is unclear, though some sources recommended to depressurise the circuit during the apnoeic period prior to removal of the preoxygenation device. Examples of how this can be achieved are:
- BVM: Dial PEEP valve to zero or disconnect the PEEP valve
- Mapleson C: Open the APL (adjustable pressure limiting) valve to zero
Disconnecting the BVM bag or the Mapleson C circuit from their connection to the viral filter is another option to depressurise the circuit, but this is not recommended due to the attendant risk of accidental disconnection of the viral filter from the face mask at that time.
Re-oxygenation between failed intubation attempts
Re-oxygenation will be most practically achieved using the same device chosen for the preoxygenation of the patient e.g. if a BVM was chosen for preoxygenation it should be used for re-oxygenation. This should be performed as a 2 person technique with a 2 handed mask grip as described above
Some sources suggest using a Supra-Glottic Airway (SGA) instead of a face mask (i.e. remove the mask from the BVM) for more effective delivery of re-oxygenation with potentially less air leak.(Alfred Guideline) However removal of the SGA for successive attempts at intubation may result in dispersal of viral droplets. Where an SGA is used, use of a second-generation device is recommended as its higher seal pressure during positive pressure ventilation decreases the risk of aerosolisation of virus containing fluid particles. (SAS)
Apnoeic Oxygenation
Summary: the balance of risks and benefits favours avoiding the use of nasal cannula for apnoeic oxygenation.
Nasal cannula with oxygen flow at 10-15L/min are generally considered routine peri-intubation care during contemporary ED intubation to extend the safe apnoea period. There is concern regarding potential viral aerosolisation to intubating staff (SAS) though it is unclear how substantial viral aerosolisation would be at these flow rates, particularly given there is dispute about the same for HFNC at far higher flow rates, albeit with staff typically located further away than intubators are.
A further consideration is that in critically ill patients with respiratory failure and shunt physiology requiring PEEP, apnoeic oxygenation may not add additional benefit as suggested by the FELLOW trial (Semler 2016). Consequently balancing possible risks and limited benefits in this population, suggests avoiding the use of apnoeic oxygenation nasal cannula.
Post Intubation Care
Summary:
- ARDSnet based, high PEEP “lung protective” ventilation was the prevailing recommendation early the pandemic although the recognition of the L & H patient phenotypes (see Oxygenation Overview section) has resulted in an alternative high FiO2, intermediate PEEP (8-10cm H20) strategy recommended for type L patients.
- The ETT cuff should be immediately inflated, prior to any attempts at ventilation post intubation to minimise expired air leak to staff.
- Consider immediate connection to the ventilator post intubation to avoid serial connections/disconnections of equipment as each poses a risk of accidental disconnection and viral dispersal.
- Do not use auscultation of the chest to confirm ETT placement and depth as this increases proximity of the intubator to the patient’s expired air without yet confirmed ETT placement.
- The ETT should always be clamped prior to any planned disconnection.
- Accidental circuit disconnection, particularly during patient transport is a high risk to staff. Consequently special care should be taken to secure points at risk of disconnection post intubation with dressing such a “tegaderm” or tape.
- In-line suction is recommended to be used within the ventilator circuit and this has significant implications for the set up of your viral filters, CO2 monitoring and timing of disconnections of the circuit.
- PPE appropriate for AGPs should be worn by any staff attending an intubated patient at all times.
Ventilator settings: the ARDSnet high PEEP “lung protective” ventilation was the prevailing recommendation early in the pandemic with low tidal volumes (starting at 6ml/kg based on ideal body weight) with high PEEP (using a PEEP-FiO2 table). However since the release of the Gattinoni paper revealing the L and H phenotypes (See Oxygenation Overview section) it is thought that while an appropriate strategy for the H phenotype with high resistance (low compliance, high lung weight and high recruitability, this strategy may have been contributing to alveolar pressure injury and poor outcomes in the L phenotype.
For the L phenotype, a high FiO2, intermediate PEEP (8-10cmH20) strategy has been advocated. Additionally, Gattinoni recommends that “once intubated and deeply sedated, the Type L patients, if hypercapnic, can be ventilated with volumes greater than 6 ml/kg (up to 8-9 ml/kg), as the high compliance results in tolerable strain without the risk of VILI.”
Gattinoni also recommends that while CT scan is the best too to distinguish between Type L and Type H patients, if not available surrogate markers can be used such as respiratory system compliance and recruitability.
The use of a tape measure to determine a patient’s height and calculate ideal body weight to avoid common overestimation of the patient’s weight and resultant excessive tidal volumes, is advocated in the LOV-ED protocol.
The ETT cuff should be immediately inflated, prior to any attempts at ventilation post intubation to minimise expired air leak to staff. (ANZICS, SAS)
For post intubation ventilation, some sources recommend immediate connection of the ventilator to the ETT (via CO2 monitor and viral filter) instead of ventilating with the BVM or Mapleson C in order to reduce the number of connections and disconnections, as each poses a risk of accidental disconnection and viral dispersal.
Confirmation of ETT placement and depth should occur through:
- Visualising passage through the cords
- Alignment of the ETT black vocal cord marker with the vocal cords.
- ETT misting
- End tidal CO2 trace
- Post intubation CXR when appropriate
Specifically, this should not include auscultation of the chest as this increases proximity of the intubator to the patient’s expired air without yet confirmed ETT placement.
The ETT should always be clamped prior to any planned disconnection.
Reports from regions experiencing high volumes of COVID-19 patients, suggest that there is a significant risk of viral dispersal to staff from the accidental disconnection of the ventilator circuit and this risk is highest during transport of the patient out of the ED. Accidental disconnections can occur at any point of the ventilator circuit between:
- Patient and ETT (extubation)
- ETT and viral filter
- Viral filter and in line CO2 monitor (if separate devices)
- In line CO2 monitor and the ventilator tubing
- Ventilator tubing and the ventilator.
Consequently special care should be taken to secure points at risk of disconnection post intubation with dressing such a “tegaderm” or tape.
In-line suction is recommended to be placed in the ventilator circuit. As this can not be provided through the viral filter, the in-line suction device will need to be placed distal to the viral filter. This can be achieved in 1 of 2 ways:
- Planned disconnection of the circuit post intubation (with attendant ETT clamping) between ETT and viral filter post intubation
- The use of a 2nd viral filter that is pre-connected (before intubation) just distal to the ventilator tubing with the in-line suction pre-connected just distal to this. Immediately post intubation, the 1st viral filter will need to be removed before connection of the ETT to the circuit. This approach has implications for the CO2 monitoring device.
- If the CO2 monitoring is provided by attachment of a sampling line to the viral filter side port, this line will simply need to be removed from 1st filter and rapidly attached to 2nd filter post intubation.
- If the CO2 monitoring is provided by an in-line monitoring device:
- This can be left in place and connected directly to the in-line suction on its distal side. The disadvantage of this set up is that the CO2 monitoring device is now distal to the 2nd viral filter which can result in clogging of the sensor with secretions (not removed through suctioning) resulting in further planned disconnections of the circuit. To avoid this, the CO2 monitor would need to be moved proximal to the 2nd viral filter immediately post intubation at the same time as the 1st viral filter is being removed.
- Alternatively the CO2 in line monitor can be pre-connected before intubation proximal to the 2nd filter but this attends a large disadvantage of not being able to use this during preoxygenation and re-oxygenation.
Due to the ever present risk of accidental disconnection of the ventilator circuit, PPE appropriate for AGPs is recommended at all times for staff attending an intubated patient.
Haemodynamic Support
Shock is uncommon (particularly pre-intubation) but if occurs, early vasopressors and inotropes should be initiated to enable a conservative fluid resuscitation/hydration strategy in order to reduce the risk of ARDS with the intermediate term goal of a negative fluid balance. (SSC, ANZICS) Early vasopressors/inotropes are most rapidly commenced by a good quality peripheral venous line (with regular monitoring of the intravenous line site) which can be converted to central venous access, if and when appropriate.
More recently it has been suggested however that the patients with the type L phenotype (see Oxygenation Overview section) may be able to tolerate more fluid than type H patients, particularly if given relatively low volumes at a slower rehydration pace (rather than resuscitation pace).
Appendices
PPE
There is variation in PPE advice between different countries. The common Australian recommendations are summarised and explained below which have been based primarily around the Australian Department of Health interim PPE recommendations for inpatients & non-inpatients, AHPPC statements on PPE (7/4/20, 24/4/20), ACEM and the AMA PPE guidelines. Conflicts between guidelines are addressed specifically in the section on Australian PPE guideline differences.
Doffing of PPE is a high risk time for staff contamination. It is recommended that both donning and doffing occur within a buddy-system to carefully observe and guide the process in an area with instruction posters also provided as a visual and memory guide. Formal, repeated staff training in PPE donning and doffing should be considered mandatory.
PPE requirements are useful to conceptualise using a 3 tiered approach. The first 2 tiers are represented in essentially all official guidelines and should be considered mandatory. The 3rd tier (suggested only for the “highest risk” AGPs) from an “official standpoint” is effectively optional as it is not specifically recommended in most official guidelines but is being utilised with a high degree of variability and heterogeneity at many health services and hospitals within Australia. Notably some overseas countries and institutions have been applying this 3rd tier more rigorously than Australia. An evidence based discussion of the 3 tier approach has now been published by Lockhart 23/4/2020.
Please note, that while some formal infection control sources don’t technically include eye protection as part of “droplet” or “airborne” precautions and instead consider this part of “standard precautions”, the practical effect of almost all guidelines has been to include eye protection as part of droplet and airborne precautions and for simplicity this has been the classification used below.
Tier 1 – For routine patient care use:
- contact precautions– long sleeved gown and gloves plus
- droplet precautions – surgical mask and eye protection (face shield or goggles)
The patient should also wear a surgical mask.
These recommendations appear based on previously known droplet spread of coronaviruses, limited evidence of COVID-19 disease spread and is supported by a recent large trial in influenza care in outpatient settings demonstrating no benefit of P2/N95 masks over standard masks in preventing infection of health care workers (Radonovich, 2019)
There is conflict between different Australian PPE guidelines regarding Tier 1 Routine Care PPE. Different guidelines recommend different exceptions to this Tier 1 Routine Care PPE. They either directly recommend, or suggest consideration of, upgrading to Tier 2 AGP PPE for routine care (i.e replacing surgical mask with N92/P2 mask) in the following situations:
- When taking swabs from a patient with fever and shortness of breath and/or severe cough (i.e as opposed to relatively well patients without severe cough) (Aus DOH recommendation)
- When providing routine care to a patient with severe acute respiratory disease/critically unwell (e.g. such as in an intensive care or high dependency unit) (ACEM PPE & AMA PPE Guidelines).
- There is evidence that such patients may produce greater viral loads with higher amounts of viral contamination detected in intensive care environments. There is no logical reason to suspect that this would not similarly apply to the same critically unwell patients being managed within ED environments.
- Staff in a COVID Assessment Clinic (based on a risk assessment)(ACEM PPE)
- Staff with prolonged direct clinical care in higher risk patient environments such as clinical areas with cohorted severe acute respiratory infection (ACEM PPE)
Tier 2 – For aerosol generating procedures (AGP) use:
- contact precautions – long sleeved gown and gloves plus
- airborne precautions – P2/N95 mask (with fit check) and eye protection (face shield or goggles)
i.e the only change when transitioning from Tier 1 to Tier 2 is that the surgical mask is replaced with the P2/N95 mask. No other additional precautions are recommended.
Tier 3 – For “highest risk” aerosol generating procedures (AGP) consider:
- contact precautions – long sleeved gown and gloves plus
- airborne precautions – P2/N95 mask (with fit check) and eye protection (face shield or goggles)
- Plus additional precautions to achieve one or all of the following 3 purposes (with examples listed):
- Maximise body coverage to better protect the neck, face, hair and wrists.
- Changes in gloves
- Use of elongated gloves to prevent gap between wrists & gown sleeve
- Use of double gloving
- Change in Eye Protection:
- Specific use of face shield instead, or in addition to goggles
- Fully enclosed goggles instead of open design goggles.
- Changes in Head/Neck protection
- Caps, or hoods
- Full body suits with hoods
- Changes in gloves
- Improve air filtration efficacy to a higher level than that provided by “fit checked” (but not “fit tested”) N95 masks.
- “Fit tested” N95 masks
- N99/P3 or N100 respirators; includes
- Elastomeric reusable half/full facepiece respirators
- Powered Air Purifying Respirators (PAPR)
- These can also provide better face +/- head covering depending on design.
- Reduce body contamination post procedure
- e.g changing scrubs, taking showers
- Maximise body coverage to better protect the neck, face, hair and wrists.
Note that:
- The “highest risk” AGPs within the ED environment generally refers to intubation.
- This 3rd tier is currently not formally advocated in most Australian guidelines as discussed above.
- There is currently high variation in Tier 3 precaution use between institutions with no accepted standard of what should constitute Tier 3 precautions – Lockhart 23/4/2020 provides one standard definition.
Arguments for and against the 3rd tier
- For:
- There is no evidence that Tier 2 precautions provide adequate protection for staff performing the highest risk AGPs. In contrast there are reports of staff being infected despite Tier 2 precautions and a plausible scientific basis that would dispute the effectiveness of Tier 2 precautions for these procedures. Given this, prioritising staff safety should result in an upgrade to some form of Tier 3 precautions. This is supported by the precautionary principle which applies when there are risks of morally unacceptable harm (staff death) based on scientifically tenable concerns.
- Staff stress and anxiety produced by the perception of inadequate protection when performing highly complex procedures (such as COVID-19 intubation) could lead to poor patient outcomes as well as ongoing risk to staff mental health.
- Against
- The use of 3rd tier precautions introduces complexity and some additional infection risks, which without proper planning and training may not reduce overall infection risk (or even increase risk):
- Additional pieces of equipment can sometimes add significant time to donning and doffing
- There can be significant risk of contamination with doffing and disposing/decontaminating some equipment, particularly without proper training.
- There can also be significant complexity regarding the disinfection of reusable items.
- Known Tier 2 PPE failures can be explained by staff error as opposed to equipment failure (although equipment failure is not ruled out and staff error may be an unavoidable systemic issue that may not be eliminated by training).
- There may be significant cost implications of implementing Tier 3 precautions.
- There may be difficulties accessing consistent supply of Tier 3 precaution related equipment.
- The use of 3rd tier precautions introduces complexity and some additional infection risks, which without proper planning and training may not reduce overall infection risk (or even increase risk):
Differences between Australian PPE Guidelines
ACEM
The ACEM PPE guidelines, while broadly similar to the Australian Government and AHPPC PPE advice, includes some key differences. Notably it contains a table that provides practical guidance regarding “PPE in specific clinical situations”.
Some differences based on this table include:
- ACEM recommends consideration of lower level precautions of surgical mask + gloves for:
- For staff not directly in contact with patients (>1.5m distance from patients at all times) who enter a cohorted isolation area (i.e: low risk encounter in a moderate risk area)
- For clinical staff in direct contact with patients screened negative or minimal for COVID risk and no respiratory symptoms (i.e moderate risk encounter with a low risk patient)
- ACEM recommends consideration of upgrading to tier 2 (PPE recommended for AGPs) in certain non-AGP “routine care” situations that are otherwise high risk encounters (based on type of contact and/or type of patient) such as:
- Staff in a COVID Assessment Clinic (based on a risk assessment)
- Staff in direct contact with patients with “severe acute respiratory infection”
- Staff with prolonged direct clinical care in higher risk patient environments such as clinical areas with cohorted severe acute respiratory infection.
For more detailed information see ACEM-PPE Guideline.
AMA
Of note, the federal Australian Medical Association (AMA) PPE Guidelines also largely conformed to federal government recommendations above but shared with ACEM the exception to the recommendation for PPE required for routine patient care, that droplet precautions should be upgraded to airborne precautions when caring for patients with severe respiratory disease (such as in an intensive care or high dependency unit).
Aerosol Generating Procedures & Events
(Adapated from SAS Consensus Statement)
| Aerosol generating events |
|
| Procedures vulnerable to aerosol generation |
|
* The reliability of seal is greatest with tracheal tube > supraglottic airway > face mask
References
- Guidelines & Resources
- Australian
- Australasian College of Emergency Medicine (ACEM) Clinical Guideline for the Management of COVID-19 in Australasian Emergency Departments
- Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group
- The Australian and New Zealand Intensive Care Society (ANZICS) COVID-19 Guidelines
- Caring for people with COVID-19 – National COVID-19 Clinical Evidence Taskforce.
- Guideline for the Intubation of Critically Ill Patients – Appendix 4 and 5: Intubation of Confirmed of Suspected COVID-19 Patients (2020 edit); The Alfred, Melbourne, Australia.
- Interim guidelines for the clinical management of COVID-19 in adults Australasian Society for Infectious Diseases Limited (ASID)
- Interim recommendations for the use of personal protective equipment (PPE) during hospital care of people with Coronavirus disease (COVID-19), Australian Department of Health
- Interim advice on non-inpatient care of persons with suspected or confirmed Coronavirus disease (COVID19), including use of personal protective equipment (PPE)
- Australian Guidelines for the Prevention and Control of Infection in Healthcare Australian Guidelines for the Prevention and Control of Infection in Healthcare, NHMRC & ACSQHC 2019
- Letter to Doctors from the Chief Medical Officer of Australia 9/3/20
- International
- Coronavirus Disease 2019 (COVID-19) Treatment Guidelines, National Institute of Health 21/4/20
- Guidance for the role and use of non-invasive respiratory support in adult patients with COVID-19 (confirmed or suspected) version 3, NHS 6/4/20
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)
- Clinical management of severe acute respiratory infection when novel coronavirus (nCov) infection is suspected, WHO.
- Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19)
- COVID-19 Airway Management Principles – joint UK society guideline.
- International Pulmonologists Consensus on COVID-19, 2020
- Australian
- Journal Articles
- Ai, T., et al. (2020). “Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases.” Radiology: 200642.
- Alraddadi, B. M., et al. (2019). “Noninvasive ventilation in critically ill patients with the Middle East respiratory syndrome.” Influenza Other Respir Viruses 13(4): 382-390.
- Fang, Y., et al. (2020). “Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR.” Radiology: 200432.
- Gattinoni, L. et al (20200 COVID-19 pneumonia: different respiratory treatment for different phenotypes?
-
Gattinoni, L., et al. (2020). “COVID-19 pneumonia: ARDS or not?” Critical Care 24(1): 154.
- Guan, W. J., et al. (2020). “Clinical Characteristics of Coronavirus Disease 2019 in China.” N Engl J Med.
- Kumar, A., et al. (2009). “Critically ill patients with 2009 influenza A(H1N1) infection in Canada.” Jama 302(17): 1872-1879.
- Jin, Y. H., et al. (2020). “A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version).” Mil Med Res 7(1): 4.
- Leung, C. C. H., et al. (2019). “Comparison of high-flow nasal cannula versus oxygen face mask for environmental bacterial contamination in critically ill pneumonia patients: a randomized controlled crossover trial.” J Hosp Infect 101(1): 84-87.
-
Marini, J. J. and L. Gattinoni (2020). “Management of COVID-19 Respiratory Distress.” Jama.
- Radonovich, L. J., Jr., et al. (2019). “N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial.” Jama 322(9): 824-833.
- Rello, J., et al. (2012). “High-flow nasal therapy in adults with severe acute respiratory infection: a cohort study in patients with 2009 influenza A/H1N1v.” J Crit Care 27(5): 434-439.
- Rodríguez, A., et al. (2017). “Risk Factors for Noninvasive Ventilation Failure in Critically Ill Subjects With Confirmed Influenza Infection.” Respir Care 62(10): 1307-1315.
- Semler, M. W., et al. (2016). “Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill.” Am J Respir Crit Care Med 193(3): 273-280.
- Yang, X., et al. (2020). “Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study.”
- Zuo, M. Z., et al. (2020). “Expert Recommendations for Tracheal Intubation in Critically ill Patients with Noval Coronavirus Disease 2019.” Chin Med Sci J.
- Other References and Useful Websites/Blogs/Sources
- EM Cases COVID Update 5/4/20):
- Emrap Live Webinars 31/3/20 and 7/4/20
- EMCRIT Wee 30/3/20 Stop Knee Jerk Intubation
- REBEL EM – Hypoxaemia a better and still safe way
- REBEL Cast Episode 79 5/4/20 COVID-19 – Trying Not to Intubate Early & Why ARDSnet may be the Wrong Ventilator Paradigm
- EMCRIT Internet Book of Critical Care – COVID-19
- https://rebelem.com/covid-19-the-novel-coronavirus-2019/
- https://criticalcarenorthampton.com/2020/03/08/covid-19-your-one-stop-resource/
- https://www.worldometers.info/coronavirus/coronavirus-symptoms/
- Vapotherm analysis
Record of Guideline Updates
This guideline is periodically updated as new information becomes available to our team (i.e is a “living guideline”). This section provides a record of updates so that people who have read earlier versions of the guideline can quickly get up to speed with any changes.
- 3/4/20
- Management of Treatment of Hypoxia and Respiratory Failure section
- Photo of “Happy Hypoxic” added with minor edits to accompanying text
- NIV & HFNC section
- Changed SAS Guideline references in line with publication of updated guideline
- Notably SAS no long advising against HFNC
- Wang 2020 study added to HFNC section
- Changed SAS Guideline references in line with publication of updated guideline
- Upgraded recommendation that all staff attending intubated patients wear PPE appropriate for AGPs
- Management of Treatment of Hypoxia and Respiratory Failure section
- 5/4/20
- Added section on potential benefits of HFNC over NIV to NIV & HFNC section
- 7/4/20
- Added section on Differences between ACEM and Australian Government PPE Guidelines.
- Added ACEM guideline reference to Imaging section.
- 8/4/20
- Added Summary section to Triage section
- Added reference to AMA PPE guidelines in Differences between ACEM and Australian Government PPE Guidelines
- 11/4/20
- Added Summary section to Treatment of Hypoxia and Respiratory Failure section
- Added Oxygenation Overview section.
- 13/4/20
- Major update to Oxygenation Overview section to include modification to early intubation approach and discussion of L & H COVID-19 phenotypes and resultant advocated changes in management
- Update to Post Intubation Care section to include alternative recommended Ventilator settings for type L pheno-type patients.
- 20/4/20
- Update to PPE section.
- Introduced the 3 tier PPE classification system, with the addition of the 3rd tier to the pre-existing 2 tiers.
- Changed the classification of droplet and airborne precautions to include eye protection for simplicity (rather than including eye protection as part of standard precautions as it is technically referred to in many official infection control guidelines.
- Update to PPE section.
- 23/4/20
- Update to Oxygenation Overview section
- Added reference to just released NIH Guideline supporting the use of HFNC over NIV, and NIV if HFNC not available.
- Added reference to Richardson 21/4/2020 demonstrating 88% mortality in intubated patients in a very large cohort.
- Update to Oxygenation Overview section
- 24/4/20
- Update to PPE guideline to reference just published article supporting the 3 tier approach to PPE by Lockhart et al 23/4/20
- 25/4/20
- Removed example of situation to upgrade Tier 1 PPE to Tier 2 for routine care being “The patient has uncontrolled coughing (letter from Australia’s Chief Medical Officer)” as this advice was subsequently withdrawn by the AHPPC in their statement on 24/4/40
Disclaimer
This COVID-19 Disclaimer is provided in conjunction with our general website disclaimer.
Due to the emergent nature of the threat to our patients and health system, the information provided is based on a review of a wide range of resources without as thorough a vetting process regarding their accuracy as would be possible in non-emergent circumstances. Additionally some information sources include collegiate conversations via a wide range of clinical and social media forums as well as expert opinion rather than established evidence (which is lacking). EDGuidelines.com does not warrant that the information is free from error or omission.
Clinicians must exercise their own judgement regarding these matters and whether to utilise this information in their clinical care of patients. In particular, it is recommended you consult updated local guidelines and consider patient specific factors in applying any of this information.
EDguidelines.com disclaims all liability for outcomes related to the use of information on this page.