GUIDELINE: Click here to access the 2025 Australian Acute Coronary Syndrome guidelines
[jointly issued by the National Heart Foundation and Cardiac Society of Australia & New Zealand]
The key change and improvement in this version of the guidelines, is the adoption of the OMI (Occlusion Myocardial Infarction) paradigm for classifying ACS. The OMI versus NOMI (Non-Occlusion MI) distinction represents a significant advance on the historical STEMI v Non STEMI distinction.
See this article for further explanation of the OMI paradigm.
OMIs are now recommended to be treated just as STEMIs have been traditionally managed – emergent revascularisation with primary PCI (percutaneous coronary intervention) or medical fibrinolysis.
Note – in these Australian guidelines the OMI has been slightly rebranded as ACOMI (Acute Coronary Occlusion Myocardial Infarction).
ACOMIs
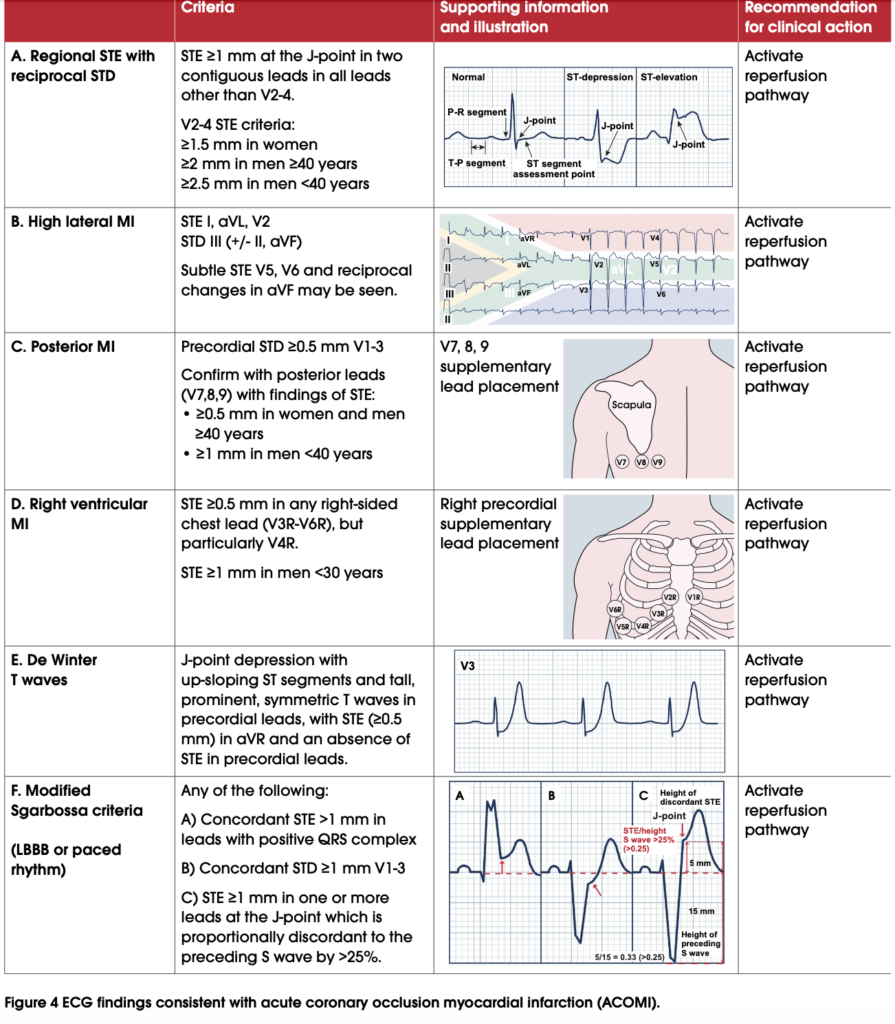
Section 1 – Assessment & Diagnosis, provides Figure 4 detailing all ACOMIs (OMIs) recognised by the guidelines as requiring management equivalent to the traditional STEMI (and includes the traditional STEMI).
High Risk ECG findings for ACS
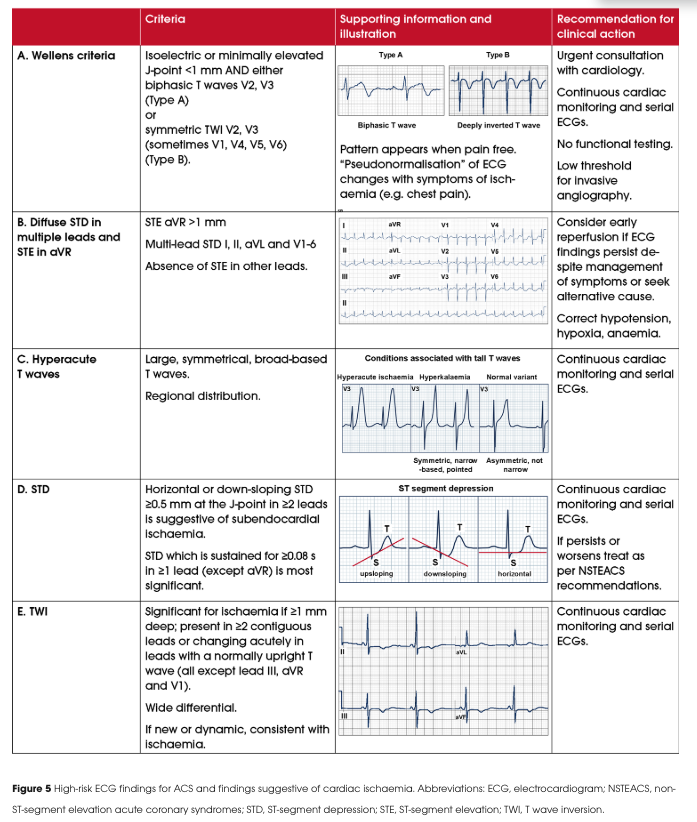
Figure 5 displays other ECG features that are highly suggestive of cardiac ischaemia and ACS. Of these, the first 3 displayed (letters A to C) are associated with “potential progression to ACOMI”:
- A. Wellen’s T waves,
- B. Diffuse ST-segment depression in multiple leads associated with ST Elevation in aVR.
- C. Hyperacute T waves
“They require prompt and continuous clinical ECG monitoring”
For further explanation and more information, see the guidelines.